
36.2K
Downloads
48
Episodes
Making Special Education Actually Work
Episodes
Sunday Jan 21, 2024
Sunday Jan 21, 2024
 Photo credit Kelly Short (colorized photo from circa 1936)
Photo credit Kelly Short (colorized photo from circa 1936)
Attention is finally being given to the effects of childhood trauma on childhood development and learning, but it's still not fully incorporated into the mainstream as common knowledge. Only when trauma-informed education becomes the norm can childhood trauma be prevented and responded-to with greater efficacy.
Because trauma often begets mental health issues, not the least of which being Post-Traumatic Stress Disorder (PTSD), and can also result in permanent physical disabilities, depending on the nature of the trauma, individuals with such impairments can become eligible for protections under disability-related laws. This includes Section 504 of the Rehabilitation Act (504), the Americans with Disabilities Act (ADA), and the Individuals with Disabilities Education Act (IDEA).
For this reason, one would think that the special education community is conducting trauma-informed assessments and considering the trauma-related needs of its students with IEPs. One would be thinking incorrectly, however. I've lost count of the number of special education assessments I've seen that are entirely silent regarding the unique traumatizing events of a student's past, like they just didn't happen or are entirely irrelevant to the assessment process, including in mental health evaluations.
I'm dealing with one of those, right now, as a matter of fact. The very signs of trauma and the historical events that likely contributed to them were described in detail to the mental health assessor, and none of those details appeared anywhere in her report. So, basically, what I took from the situation was that some ding-dong baby doll who fell out of the lap of luxury and into a master's degree in social work was dispatched to assess a student with some pretty significant symptoms who had previously lived for 11 months with her mother in their car and who had also witnessed her mother getting mowed down in the street by a car while they were crossing the street together at a protected cross-walk, leaving this student as a young child to scream for help in the middle of the street. None of these past traumatic events were discussed in the assessment report, nor were any of the symptoms that had been brought to the assessor's attention. She interviewed the student once via Zoom and noted that the student wasn't very forthcoming, and relied on classroom observations conducted by a school psychologist, who is not a mental health clinician.
Thankfully, once it was brought to his attention, the involved school district's special education director was just as taken aback as I was and immediately agreed to fund an Independent Educational Evaluation (IEE) in mental health at public expense, which is basically a second opinion conducted by an outside, uninvolved provider, that is funded by the District. We're in the process of finding an outside assessor to conduct it, but we expect the situation for this student to be resolved once it's done. However, this was just the latest of several cases we've worked in this same District over the last 15 years in which trauma and mental health issues are not being properly considered, and it's a problem that is not unique to this particular district. It seems to be a fairly systemic problem in cases we encounter from around the country.
So, I want to focus on what trauma-informed special education assessments and programming look like in actual practice, and how the applicable science and law come together around trauma-related special needs that require 504/ADA accommodations and/or IEPs. I first want to direct you to the peer-reviewed research, starting with the article, "Considerations for Incorporating Trauma-Informed Care Content within Special Education Teacher Preparation and Professional Development Programs," which appeared in Vol. 1 No. 2 (2021) of the Journal of Special Education Preparation, the full text of which is available for free online.
I think this article does a good job of explaining what it means to incorporate Trauma-Informed Care (TIC) into special education, so I'm not going to do a lot of rehashing, here. One of the things I like about this article is that it doesn't just speak to special education as a stand-alone entity; it discusses the application of trauma-informed care within an evidence-based Multi-Tiered System of Support (MTSS), such as that found with Positive Behavioral Interventions and Supports (PBIS), which are meant to catch students before they fall too far behind and provide them with whatever types of supports they need to be successful, whether through special or general education. This naturally lends it to speak to the related "child find" issues.
This article cites other researchers by saying: "... adverse childhood experiences (ACEs; Felitti et al., 1998) ... are all common experiences for students with emotional/behavioral disorders (Cavanaugh, 2016)." Certainly, one way to identify children who may need special education as per "child find" is to look at those already known to have experienced ACEs to determine if they are showing any signs of emotional and/or behavioral disorders. The moment it is known that a general education student has survived a traumatic event, a special education assessment referral should be made and it should include sufficiently comprehensive mental health evaluations to accurately capture any impact the traumatic event has had on the child's ability to access and participate in education. Even if the child ultimately does not qualify for special education, Section 504 relies on the special education process to gather its own assessment data to inform appropriate 504/ADA accommodations for children with disabilities who do not require special education.
If the child is unavailable for learning due to extreme trauma, then the interventions have to restore the child to the point of being available for learning again, unless the child is medically incapacitated. If medical interventions are first necessary, those obviously come before any special education or 504/ADA accommodations. A child has to be physically medically stabilized before they are available to participate in education and anyone can know what to do for them at school. New assessments will have to be done to determine the student's new baselines once physical medical stability is achieved.
If the child is psychiatrically incapacitated, it may be necessary for that child to be placed in a residential psychiatric treatment facility with an onsite school in order for the child to become available for learning. I'm not a huge fan of residential placement, but there's a time and a place for everything. I've had a number of students benefit tremendously from a special education residential placement for these kinds of severe mental health needs, though I've also had students on my caseload molested and assaulted in some of the residential programs, so this model of intervention is hardly a monolith or panacea.
The above-cited article makes the following recommendations: "Considerations for special education professional development includes teachers undergoing an extensive training that addresses the following components:
- Understanding Trauma and ACEs (Dong et al., 2003)
- Challenging current thought processes vs. TIC attributions (Hoskins et al., 2018)
- Identifying ways educators may be trauma informed (Plumb et al., 2016)
- Direct overview of MTSS (August et al., 2018)"
Understanding Trauma and ACEs: School site staff who do not have a professional understanding of what trauma is, what ACEs are, and how they affect student performance are at a gross disadvantage when it comes to actually serving the public good. The pervasiveness of trauma in everyday life, anymore, is something we all have to consider when dealing with each other. We should certainly be able to expect our professionals who encounter it in the field daily to have an intelligent plan of action for how to respond to it appropriately in their professional capacities. We shouldn't be ending up with privileged ding-dongs with fancy degrees who can't recognize what they're looking at when they encounter childhood trauma in the field.
Challenging current thought processes vs. TIC attributions: Long-entrenched policies and practices that fail to meet the needs of certain populations are effectively institutionalized biases against them. In professional settings in which no policies and procedures exist to appropriately respond to the needs of students who have experienced ACEs and trauma, there is no institutionalized response to proactively address the situation, which becomes an institutionalized proactive effort to ignore it. When people feel powerless to help someone being hurt by something, it's a natural psychological defense mechanism for them to blame the victim for deserving mistreatment rather than live with feelings of helplessness, powerlessness, cowardice, or whatever else feels bad that goes along with not helping. Victim-blaming is meant to offset feelings of guilt for not helping.
Too often, adults in the public school setting become angry at children for manifesting the symptoms of trauma and ACEs, punishing them instead of helping them and making a bad situation worse. There is no excuse for this kind of conduct in a professional educational setting, and certainly not in this day and age when there is plenty of peer-reviewed research capturing strategies and approaches that actually work. As I've said in other posts, however, there are no real mechanisms in place in public education at this time for the consistent promulgation of the peer-reviewed research among the educators to equip them with the resources to translate the research into actual, practical classroom applications.
Where parents really need to get vocal at their school board meetings is in advocating for the application of the peer-reviewed research to the design and delivery of public education. It's not like we don't have evidence of what works. Education research continues to compile and accrue over time into an ever-enriching body of knowledge that can be used to solve so many of the world's ills that it should be a crime that it's not already being actively applied by competent professionals throughout the public education system on the regular.
Identifying ways educators may be trauma-informed: It seems that using logic models has been the most effective way to communicate concepts around identifying ways that educators can become trauma-informed. The School District of Philadelphia has created a logic model that serves as a useful example, which is illustrated below.
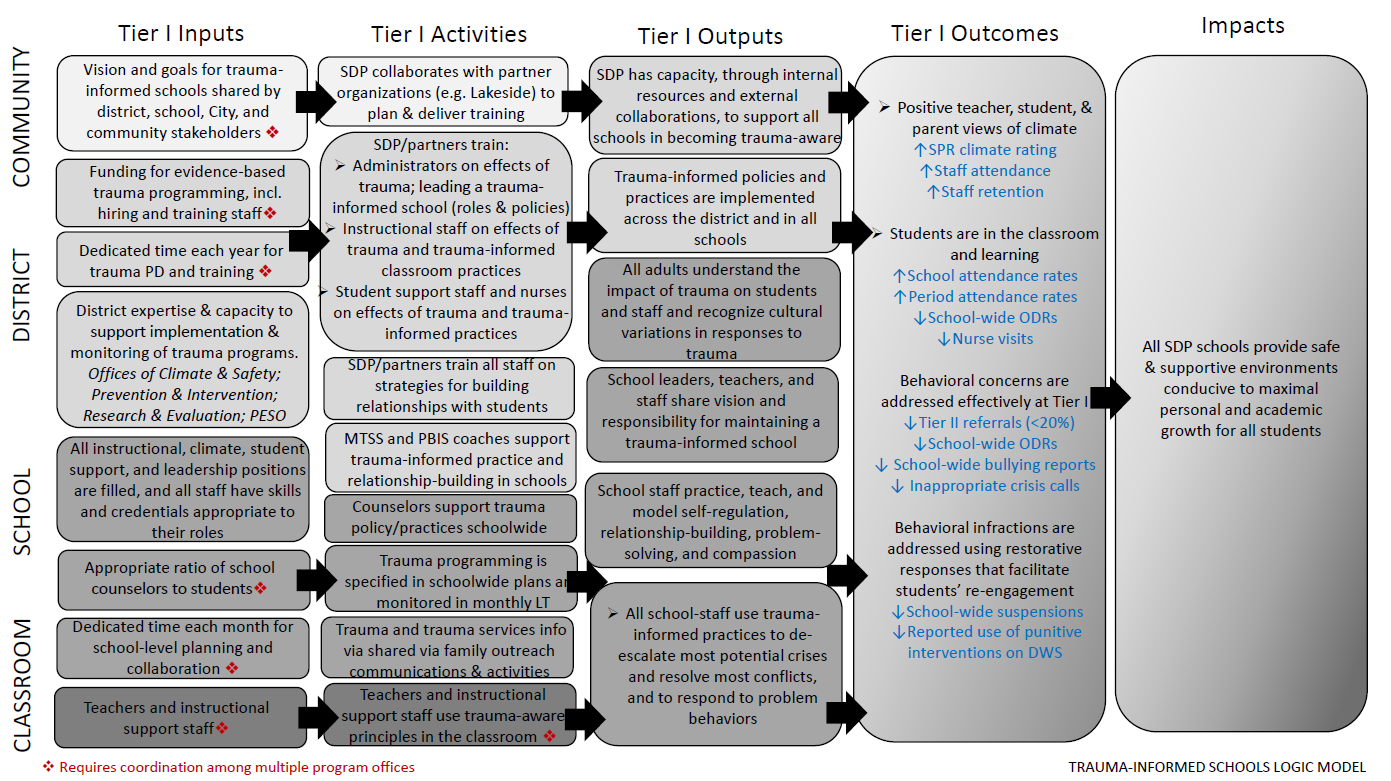
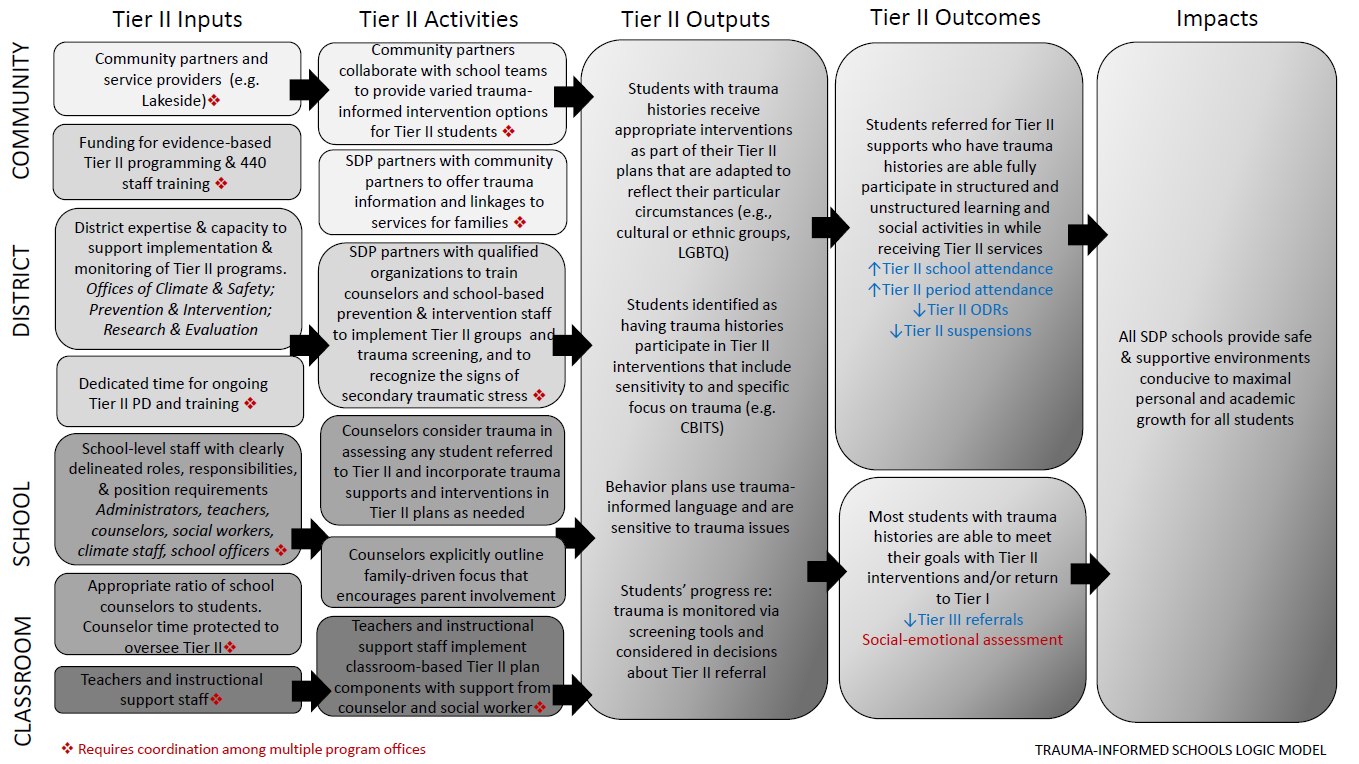
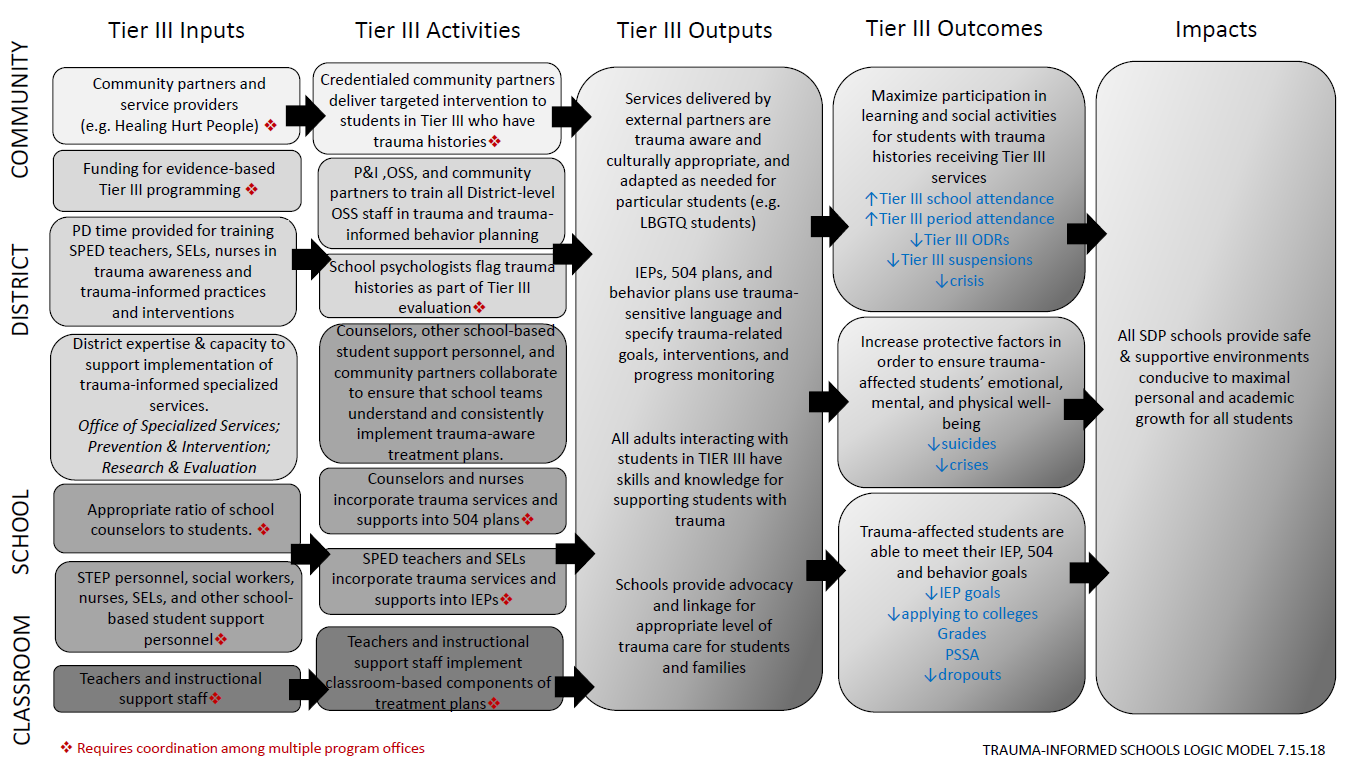
You can look at this logic model more closely by clicking on the images or the link in this post. What you can see once you look at it is that the District's MTSS incorporates TIC into its design. I can't speak to the fidelity with which The School District of Philadelphia actually abides by this design or the degree to which it works. I can only show it to you as an example of how to create this kind of a design, which requires staff to be trained on how to implement it in order for it to actually work. By creating this kind of operational framework and training everyone within the school site on how to carry it out, staff become informed on what to look for and what to do when they see it, when it comes to trauma and its potential for undermining student learning.
Direct overview of MTSS: The above example shows how TICs are woven into an existing MTSS. Very often, special education personnel don't understand where they fit into the overall tiers of intervention, and usually because the rest of their co-workers and superiors have no idea, either. None of these MTSS designs will work if staff don't recognize themselves in all of the pieces of the design for which they are each actually responsible. It's not enough to create a pretty logic model on paper. The logic model has to actually be executed according to its design or it's worthless. To that end, it is imperative that both general and special education staff understand where the lines are drawn between their two universes and a child needs to be referred for special education assessment.
I actually have a case from my past that I can refer to as an example. In this case, the district had some kind of MTSS but it had failed to work in special education and the "child find" process in any kind of meaningful way. As such, staff didn't know their roles when it came to "child find" and made mistakes all over the place. This was a case of multiple ding-dongs who had no idea what they were doing, trying to fake their ways through the MTSS design process and botching it royally. What's worse is that the involved student in this example was being raised by his grandmother, who had been a teacher for this same school district for over 30 years at the time of this hearing, and her daughter, the student's mother, had gone on to become a teacher of the same district, as well. The employees of this district were doing this to each other's families, and purely out of ignorance and a grotesque leadership failure.
When done correctly, a school- or district-wide MTSS that incorporates TIC will naturally lend itself to helping those children who need special education mental health supports for any reason. Investing in developing a high-quality MTSS that incorporates TIC will appropriately funnel the children who need special education mental health services into the appropriate levels of intervention relative to their unique, individual needs.
That said, it's not enough to simply refer children suffering from mental health issues related to trauma for assessment. The quality of the assessments conducted matter and leaving out critical information about the trauma a child has already experienced and how it is affecting that child's learning is a fatal flaw that compromises the validity of the assessment and gives the parents a legitimate reason to disagree and request IEEs at public expense.
Administrators looking to cut corners will often try to minimize costs by having school psychologists do some basic social/emotional assessments instead of having proper mental health evaluations done by licensed mental health providers. This is no place to be cutting corners. First, it saves no money in the long run. Pretending the problem isn't as bad as it actually is will blow up in your face, eventually. The longer the problem goes untreated, the harder and more costly it will become to address later on. Secondly, it's heinously unethical. What kind of a person do you have to be to deny necessary mental health services because you don't want to spend the money? Any school district administrators who think their budgets are more important than the lives of their students shouldn't be employed in public education. The budget exists for the benefit of the students, not the administration. For that matter, school district administrators exist for the benefit of students; students do not exist for the purpose of lining administrators' pockets with unearned tax dollars.
I know the technical issues of how to integrate TIC into a schoolwide system of successful interventions is a topic worthy of a full-day workshop and I'm not doing justice to the entire issue, here. But, I'm hoping that I've given you enough to think about TIC in special education and some pointers towards some resources that can help you as a parent, educator, and/or concerned taxpayer to address these kinds of challenges. We need to appreciate the degree to which special education can be a tool to protect our local communities and national security from unstable individuals responding to their personal traumas in ways that can hurt many other people in addition to themselves. In this day and age of mass shootings by people suffering from significant mental health issues, we can't neglect to preempt these behaviors where we can by intervening in the lives of children who experience trauma and/or have mental and emotional health needs that affect their access to learning and behaviors. It takes a village to raise a child, and this is how it's done when the child has experienced trauma.
No comments yet. Be the first to say something!